The Biggest Mistake You're Making With Menopausal Hormone Replacement (MHT) and What to do Instead


The treatment of symptoms arising from the menopausal transition and the prevention of future health problems with menopausal hormone replacement (MHT) are exploding areas of interest these days, which is no bad thing. Women's health has long been neglected by Industrial medicine. For example, it's only in the last few years that female mice are beginning to be included in research, their estrous hormone cycle introducing annoying complexity into research compared to their more straightforward, non-cycling male mice counterparts.
Better to keep it simple and use only male mice to study health, the thinking went. And then apply what we learn from researching male mice to everyone.
The other bit of important context for the massive growth in interest is a gigantic menopausal hormone therapy (MHT) pendulum swing we're currently witnessing.
Starting in the 1940's, hormones had been prescribed to perimenopausal women to counter-act symptoms like hot-flashes, night sweats and mood swings. The number of prescriptions steadily rose until climaxing in the early 2000s.
There had been concerns around MHT safety from the outset, including the increased risk of ovarian and breast cancer with using estrogen on its own without progesterone. But in 2002, the poorly designed Women's Health Initiative (WHI) study was published, which found increased risk of harms such as blood clots, heart disease, and stroke. While the study had many flaws and the harms were exaggerated, the results led to a drastic decline in prescriptions.1
What we're now seeing are those who are rightfully critical of the misinterpretation of the 2002 WHI results coming out in full force promoting MHT as the best thing since sliced bread, with some arguing that it's actually dangerous not to replace hormones after menopause to prevent bone thinning and cognitive decline, a concern that I hear often from patients.
Without going into the details of the trial, what I will say is that it both can be true that the WHI study was flawed and misinterpreted and that MHT still comes with risks that are being down-played. I believe that's likely the case.
However, what I'd like to focus on here is the biggest and perhaps most easily addressed problem I see women making when it comes to supporting hormones around peri- and post-menopause: supplementing hormones while in an inflamed, hormone-resistant state. In other words, timing.
Putting the Cart Before the Horse with MHT
By far the biggest mistake that I see women making with MHT is the timing of when they're considering using it. What has been completely overlooked in the discussion of female hormones around peri-menopause is what is commonly happening with female hormones in the decades leading up to The Change.
The commonly told story is: in your fertile years, you have estrogen and progesterone cycling throughout the month. When you go through menopause, this goes haywire and then stops all together, leaving you in a dangerous, hormone deficient state, that can only be corrected by taking hormones.
First, the majority of our sex hormones are actuallly intracine rather than endocine, which means that they are made and used inside of cells and are not measured on regular blood tests.2 This reminds me of the old story of the drunkard who lost his keys and looks for them under a streetlamp. A policeman comes over and asks him what he's doing. The drunkard says he's looking for his keys. "So you lost them here under the street lamp?" "No," the man replies. "I lost them way over there in the field but the light over here is better."
We focus on hormones in serum because that's what we can easily measure. The hubris is then assuming that what we measured is representative of what's going on globally. But most of the action is occurring in places in the body not reflected labs.
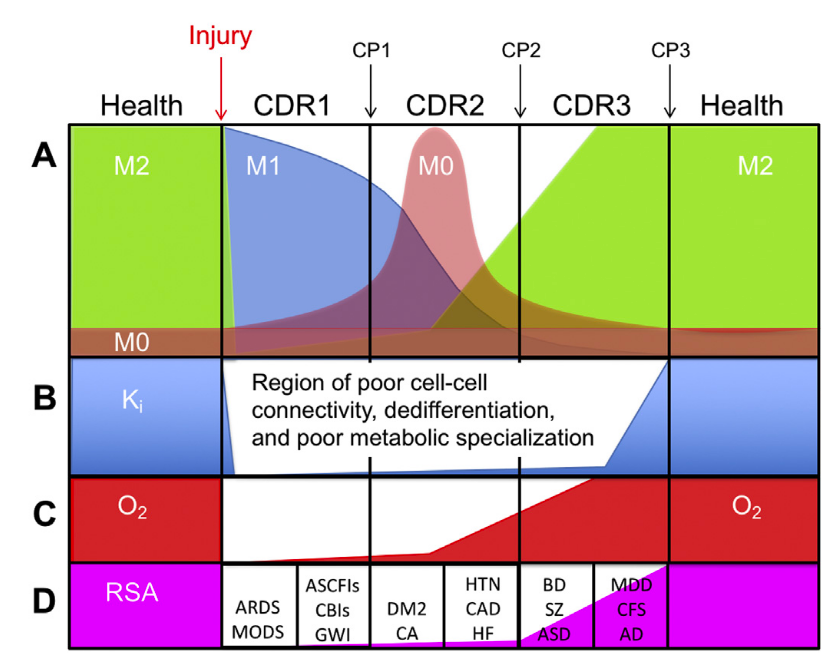
The next problem is that low hormone levels in serum, even if they did represent systemic levels, which they don't, are still badly misinterpreted. When cells are stressed or inflamed, they kick into a healing mode called the Cell Danger Response, a 3-step process that involves inflammation, tissue repair, and network re-establishment.
A necessary requirement of the Cell Danger Response is creating hormone-resistance in target tissues and reducing the production of hormones centrally.
Why would your body choose to do this? Because when you're healthy, the body is coordinated centrally by the heart and brain. But if, let's say, you have an infection, injury or other local stressor, the body switches into a more primitive mode to allow affected tissues to be regulated and acted on locally in order to combat infections and heal tissue, rather than regulation from afar by the distant brain.
When a local disaster strikes, the focus becomes local. Rather than what's going on at distant, centralized locations.
Endocrine hormones are substances that act on distant tissues. And so in order to give inflamed tissues the autonomy they need to heal, hormone resistance is induced temporarily to facilitate healing.
Of course, when stress and inflammation are chronic, then hormone resistance becomes chronic, too.
Here is a rather long, but very important and worthwhile quote from Bob Naviaux's seminal paper: Metabolic features and regulation of the healing cycle—A new model for chronic disease pathogenesis and treatment:
"End organ resistance to hormone signaling is an intrinsic part of the CDR. Once a tissue suffers injury, a shift to dependence on local chemical cues and paracrine signaling is essential. Remote decision-making by endocrine glands cannot provide "boots on the ground", real-time instructions to injured cells when bidirectional lines of communication are disrupted. A shift from fully integrated and periodized metabolism to cell-autonomous metabolism is an obligate feature of CDR stages 1 and 2. . .
Thyroid, adrenal cortical glucocorticoid and mineralocorticoid, and renin-angiotensin system attenuation states are common in patients with chronic fatigue syndrome (CFS). The most common forms of stimulus-response dysregulation lead to complex endocrine syndromes that do not fit classical medical definitions of deficiency or failure because residual hormone production can usually be shown by physiologic stimulation, but is suppressed. These complex disorders have sometimes been called thyroid or adrenal exhaustion syndromes.
In all these end-organ resistance states, the treatments that have been most effective are metabolic, diet, and lifestyle interventions that restore normal bidirectional function of the endocrine system. In contrast, chronic treatment with the hormone in question typically leads to iatrogenic side-effects, and dependence on the exogenous hormone. Knowledge of the cell autonomy requirement of the CDR helps reframe the causal mechanisms behind these previously unconnected syndromes."3
The key things to understand is that hormone resistance induced by triggers such as infections, toxic chemicals, artificial lighting, non-native EMFs, and other threats is a feature, not a bug. I believe that understanding this fundamental aspect of hormone regulation is crucially important for those trying to navigate the important yet confusing world of hormonal health.
I also believe understanding fundamentals like this should be the price of admission for even considering tinkering with these levels pharmacologically.
What's more, when cells are stressed and enter the Cell Danger Response, detoxification is essentially paused in favor of defense and survival. So while we're entering a state of being less hormonally sensitive and perhaps producing lower levels centrally, we're also not clearing our used hormones as efficiently, which also contributes to hormonal dysregulation.
What this means is that when it comes to MHT, the discussion has been mainly around whether or not to do it. Whether it's good or bad. Like most things, the Devil's in the details and true understanding comes from nuance, not black and white thinking. Timing has only entered the discussion around when to do it as it relates to the hormonal transition - before, during, or after menopause.
But the distinction I'd like to make is that aside from whether your cycle is regular, irregular and completely stopped altogether due to menopause, you would do well to address inflammatory triggers and hormonal regulation before considering "topping up your levels" (at least the ones we can measure on lab tests, which isn't most of them). And you may very well find that many of the symptoms you were attributing to "hormone deficiency" self-correct when you address the inflammatory triggers that were leading to hormone resistance and improving hormone regulation and sensitivity.
How do I know you're inflamed? Well, I don't. Not really. But according to a 2022 study, only 6.8% of US adults have optimal cardiometabolic health. This data includes both men and women and all adult age ranges. But even if we focus just on 20-34 year olds, over 80% of them had cardiometabolic problems and inflammation.4
So statistically speaking, I'm pretty confident that looking for and resolving triggers of inflammation and stress are likely higher leverage and less likely to cause unintended harm than starting by asking whether to administer MHT by cream or a suppository.
Are Hormones Really the Best Way to Address Hormone Deficiencies, anyway?
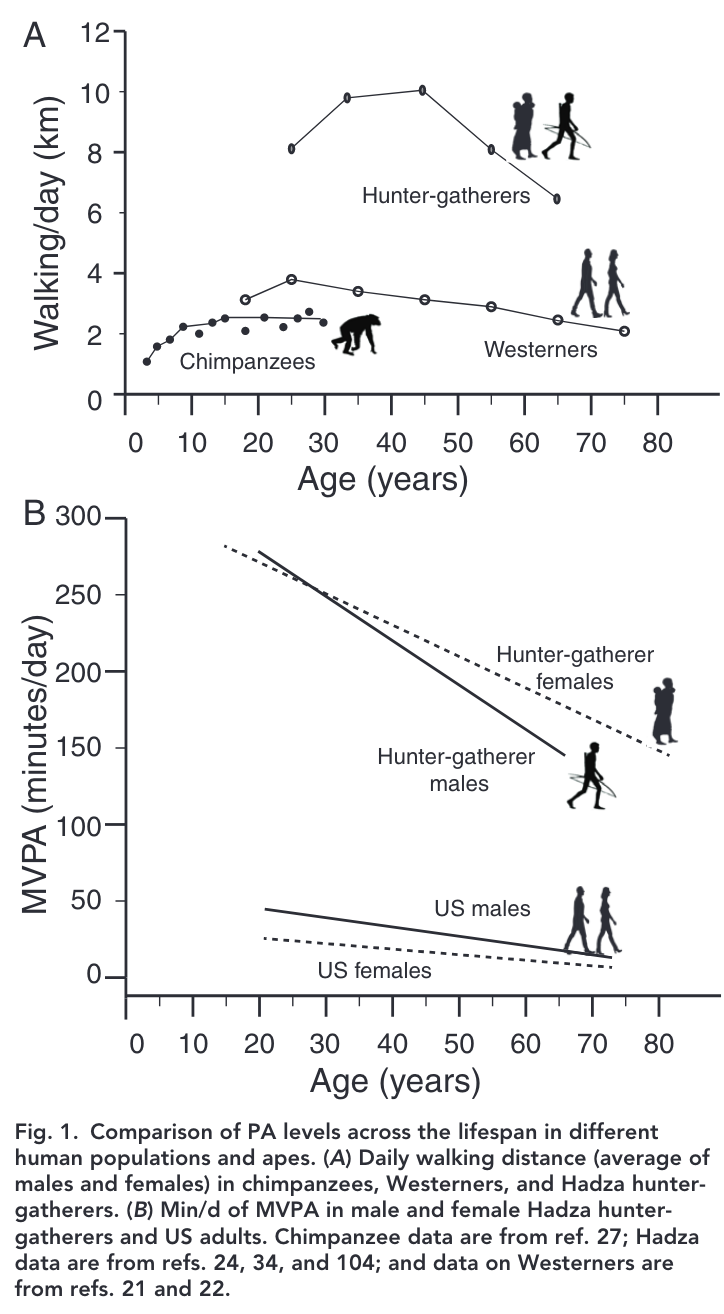
So we've addressed the assumption that the symptoms that commonly come around menopause are caused by hormone deficiencies inherent in this transition, despite the fact that pre-industrial women lived in optimal health for decades after menopause.
(As an aside, there's a widely circulating myth including in the somewhat ironically named "The Great Menopause Myth" that it was uncommon for women to go through menopause before the 20th century, that prior to modern times "menopause was death" and this misconception is used to argue that all post-menopausal women are essentially sick if they don't take supplemental hormone. This misconception is due to authors and hormone influencers mistaking "life expectancy at birth", which takes into account childhood mortality and is typically a much lower average age, with "typical lifespan", which is the average age that adults live to once they reach adulthood. Humans have had a significant post-reproductive, healthy and active lifespan for between 150,000 and 1.6 million years.5 )
In reality, an intrinsic part of chronic inflammation, by the very nature of how it works, induces hormone resistance and intentionally lowered production of hormones. The overwhelming majority of women are affected by this compensatory hormone resistance state prior to the menopausal transition and they may do better to address these issues before considering MHT.
But is MHT the best option for most women wanting to boost their hormone levels? Is it the only option?
Well, Chinese herbal medicine has been addressing endocrine issues including those brought on by the menopausal transition for thousands of years. Humans have co-evolved to use botanicals for a significant part of our evolution. Skeptics might argue that longevity doesn't demonstrate efficacy, although both research and common sense tell us otherwise. Whether or not a practice is helpful is a central factor in its longevity.
But fortunately, we actually have a whole literature looking at metabolomics, randomized trials and other clinical studies showing sophisticated pharmicodynamics of various commonly used formulas that have the clinical benefits associated with hormone replacement without the off-target effects, such as endometrial thickening that can be a precursor to cancer, common with exogenous estrogen.
The best real-world data we have is from a 2024 study conducted in Taiwan, where pharmaceutical MHT and Chinese herbal medicine are both regularly used within their national health service. Looking at over 12,000 women, they found that those who used herbs had a 40% lower risk of developing cancer and a 60% lower risk of all cause mortality compared to those using pharmaceutical MHT.6 They also found that the safety difference was apparent after only 6 months of use.
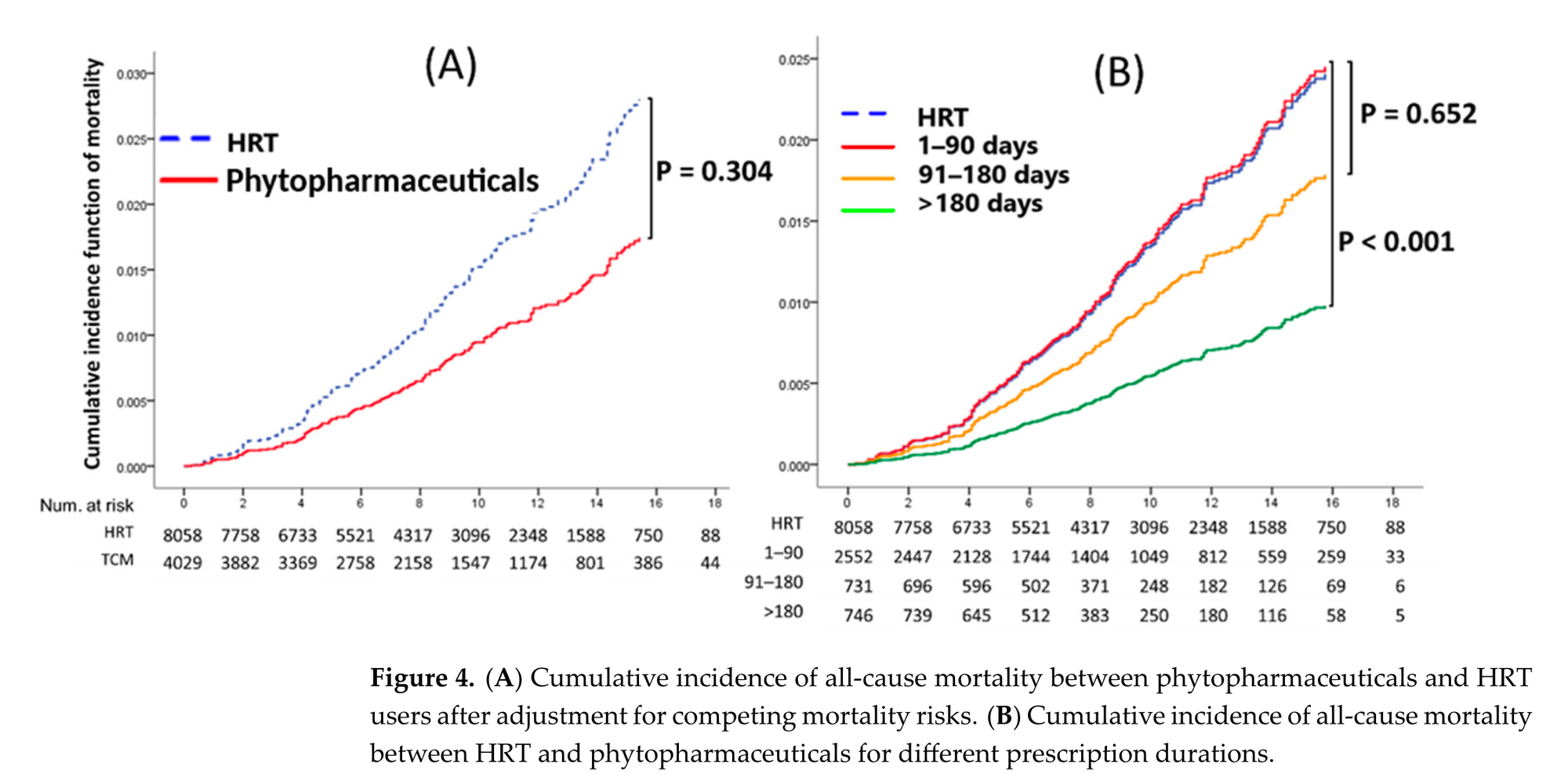
This suggests that MHT causes cancer and death or that Chinese herbs are much better at preventing these outcomes or some combination of both. Yes, in this study design like all study designs, there can be sources of bias, as it wasn't a randomized placebo-controlled trial but rather a population-based cohort study. But if the results are indicating a placebo effect, the magnitude of safety provided to those who received herbs or those harmed by receiving MHT still merits a further look.
That said, based on the literature as a whole, including safety studies on MHT and metabolomics research into herbs, it's far more likely that the bulk of these findings are due to a true effect.
What I suspect is that the clinicians, influencers and hormone-expert practitioners, all doing great work and very well meaning, recommend hormones rather than herbs because they are simply unaware of these other tools. Part of my intention here is to increase that awareness.
I first started running hormone tests and recommending bio-identical hormones over a decade ago. At the time, I believed what I was doing was precise, cutting-edge, individualized and far more sophisticated than what herbal formulas can achieve. Now that I've studied the literature and frameworks around Chinese herbal medicine and have had time to see how women respond, I've found that most of the time, these tools can provide better benefits with fewer risks for most women.
And when hormone replacement is used, as part of an appropriate clinical order of operations, women often find benefit at lower doses of hormones and find that MHT works better for them.
Parting Thoughts
Hopefully this provides some helpful context on avoiding the pitfalls of navigating the menopausal transition by starting with MHT out of the gate by understanding some basics around hormonal imbalances that the vast majority of women face prior to menopause. Clinically, whether it's for complex chronic health challenges or general hormonal health, I guide people through a 5-Stage process that begins by removing immune triggers in Stage 1, resolving digestive inflammation in Stage 2 and improving hormonal regulation in Stage 3, before considering hormonal supplementation in Stage 5, if it's needed at all.
More importantly, by learning how to navigate a step-by-step process for health creation, you learn how to interpret your body's feedback so that you can figure out exactly what's working for you, based on accurate frameworks and research.
References
- Prentice, Ross L., and Garnet L. Anderson. "The women's health initiative: lessons learned." Annu. Rev. Public Health 29.1 (2008): 131-150.
- Intracrine Regulation of Estrogen and Other Sex Steroid Levels in Endometrium and Non-gynecological Tissues; Pathology, Physiology, and Drug Discovery Gonda Konings 1,2t, Linda Brentjens 1,2t, Bert Delvoux 12, Tero Linnanen?, Karlijn Cornel 1,2, Pasi Koskimies®, Marlies Bongers 1,2, Roy Kruitwagen, Sofia Xanthoulea and Andrea Romano ↩︎
- Metabolic features and regulation of the healing cycle-A new model for
chronic disease pathogenesis and treatment
Robert K. Naviaux ↩︎ - Trends and Disparities in Cardiometabolic Health Among U.S. Adults, 1999-2018. Meghan O'Hearn, MS," Brianna N. Lauren, MS," John B. Wong, MD,b, David D. Kim, PHD, Dariush Mozaffarian, MD, DRPHa,b ↩︎
- Gurven and Kaplan. Beyond the grandmother hypothesis: evolutionary models of human longevity, 2008 ↩︎
- Comparing Cancer Risks and Mortality between Phytopharmaceuticals and Estrogen-Progestogen Medications for Menopausal Women: A Population-Based Cohort Study Tsai-Bei Lin 1, Chia-Chi Hsieh 2,3,t, Chun-Hsiang Wang , Chiung-Hung Chang 5, Yu-Ling Hsueh 6, Yuan-Tsung Tseng 7, and Men-Fong Hsieh 6,* ↩︎