Dear Science Based Medicine, Just a Few Questions About Acupuncture


The folks at the Society for Science Based Medicine have some strongly negative views about acupuncture. I’m fairly sure that none of them have actually tried it, but acupuncture sounds pretty unscientific, doesn’t it? Anyways, I’m sure they’re right about everything (groups with ‘Science’ in the title always are) but I just wanted to get clarification on a couple of things.
Dear Science Based Medicine, I have a few questions about acupuncture:
First, I just want to start by saying that I am a long time reader and a huuuuge fan of your blog. I simply love love love (!) your thoughtful, witty, and thorough treatment of all things science based and medical! Please keep up the good work.
I just have a few questions. You write an awful lot about acupuncture and you obviously know a lot about it. It’s clear from reading your posts that it definitely doesn’t work. That’s for sure. It was really helpful for me to get clear on this since I’m an acupuncturist.
I now understand that the positive results I see in practice are due to the subjective impression of improvement without actual improvement and the lack of a controlled setting and basically people in general being, how do you describe them? Kinda simple and a bit moronic? I mean, people actually think that they’re in less pain, sleeping better, feel better in themselves, pooping more when they were constipated, pooping less when things were moving too quickly, taking less medication, and taking fewer days off of work, etc etc. What a bunch of gullible dodo brains, am I right? That post hoc, ergo propter hoc gets them over and over (and over and over) again. Poor dears.
Anyways, I hope you don’t mind, but after reading your various articles on acupuncture, I just have a few questions.
Defining Acupuncture: to Qi or not to Qi?

On your site, you define acupuncture as “the practice of placing very thin needles through the skin in specific locations of the body for the purpose of healing and relief of symptoms.” I think this is a good definition, pretty standard and agreed upon. After all, no matter what style is being practiced or strange rationale for choosing points, etc, that is exactly what acupuncture is.
But when you say that acupuncture doesn’t work, the main argument you repeat over and over (and over and over again) is that acupuncture doesn’t work because there’s no such thing as qi. I think the question of whether or not there’s any basis for the existence of qi is a fascinating topic myself, but totally irrelevant in this context, as it addresses the rationale not the effectiveness of the intervention. Whether or not inserting and stimulating small needles for therapeutic benefit is effective for symptom reduction or disease resolution really doesn’t rely on the existence of qi as an explanatory model. I’ve learned a lot about logical fallacies (and a smattering of Latin) from your site, and I think this is what you would call “argumentum ad dictionarium“ where you rest the support for your claim by changing the definition of what you are describing.
So, when you say that “without chi, there is no underlying basis for acupuncture as a medical intervention,” well, isn’t that a bit silly? You’re basically saying that in order for sticking needles into someone to have a therapeutic effect, then qi must exist and if qi doesn’t exist, then acupuncture has no therapeutic benefit. Isn’t that what you logicians call a non sequitur? I mean, I may choose to needle Gall Bladder 41 for my patient’s migraine because it’s the 3rd Tuesday of the month coinciding with a Harvest Moon while Mercury is in retrograde whilst sporting a tiara and doing the Hokey Pokey. But, none of that directly addresses the issue of whether or not my patient’s migraine went away. (Oh, how I do love Tiara Tuesdays . . .)
So when you sweep the vast amount of biological research into acupuncture’s mechanisms under the rug by saying that “it is misleading to say that such mechanisms could explain ‘acupuncture,’” well isn’t that only true if you define acupuncture differently from how you originally defined it? I mean, if we use your definition of acupuncture as “the practice of placing very thin needles through the skin in specific locations of the body for the purpose of healing and relief of symptoms” as you did, then isn’t this vast body of research into the effects of placing very thin needles through the skin the epitome of relevant for the question at hand?
Biological Plausibility: the dizzying merry-go-round of circular reasoning
One of your main arguments against acupuncture is that it “lacks a plausible mechanism.”
But you also argue that the copious amount of research into acupuncture’s mechanisms is “not relevant to the argument” of whether or not acupuncture works. I find this really confusing because you say that “[b]asic science considerations are, in essence, ignored in determining whether there is sufficient prior scientific plausibility of acupuncture to treat, for instance, infertility (1) or depression (2), and equivocal, bias-prone clinical trials are ranked much higher than the basic science considerations that make the hypothesis that acupuncture can do anything for infertility so implausible as to border on impossible, barring new evidence speaking to its plausibility.” (Gorski)
So, if I understand you correctly, you’re saying that acupuncture as a treatment modality is implausible but you’re not going to look at the research that explores its plausibility because it’s irrelevant to the argument? In order to take a “science-based” approach to the question of acupuncture’s biological plausibility, you are going to make a conscious decision not to evaluate the research into its effects on the brain using fMRI studies,3 4 5 purinergic signalling,6 7 autonomic tone using heart rate variability,8 9 effects on gene expression using high throughput metabolimics,10 and mechono-transduction studies11 compared to sham. That’s an interesting stance to take.
Actually, I take that back, you did address purinergic signalling when you discussed Goldman et al’s 2010 study on the effects of acupuncture on adenosine in mice.
You deemed this study to be of very high quality but sadly misinterpreted by the study authors and the media. The consensus was that this study supported a potential mechanism for acupuncture analgesia. Your more reasonable interpretation? “This study actually says very little about acupuncture. What this study shows is that sticking needles in mice causes adenosine production and that that adenosine can blunt the pain response in nerves by binding to the A1 receptor. Nothing more.”
Wow, that’s a very . . . nuanced position. I feel relieved that the good people of Science Based Medicine are equipped to tease out these subtleties. Here was the scientific community interpreting this study as elucidating a mechanism for acupuncture analgesia via adenosine signalling, but really it says nothing about acupuncture, only the insertion of tiny acupuncture needles. It’s gems like these that make reading your blog so illuminating!!
So acupuncture lacks a biologically plausible mechanism but any studies that contradict this viewpoint are “irrelevant to the argument.” Any mechanistic studies about acupuncture that you have managed to read that do show a plausible mechanism don’t actually address acupuncture, just the insertion of tiny acupuncture needles in an acupuncture treatment-reminiscent fashion. Got it.
To bring this pony ride full circle, you have then found an ingenious recipe for erasing the significance of positive clinical trials by waving the magic wand of “prior plausibility.” I say it’s a magic wand because it’s subjectively and arbitrarily, not mathematically, determined – in this case, by people who consider the literature that would allow them to reasonably determine prior plausibility “irrelevant” and have instead decided to go with their gut on this one.
By assigning a low prior plausibility score to acupuncture, any positive studies now magically have very little positive predictive value – in other words the chances that a positive study is a true, rather than false positive, are inversely proportional to the prior plausibility value that you made up off the top of your head without reading the literature!! Bravo!!
Pragmatic studies – Better to be a skeptic with a migraine than a pain free idiot, am I right? (Up high!!)

Regarding pragmatic studies, where two treatments go head to head in the real world, you explain that “[p]ragmatic studies are useful for the questions they are designed to answer: how a treatment performs outside the limited environment of a research study, which of two treatments should be preferred by doctors, patients, and policymakers, deciding how limited resources can be best utilized. They are an integral part of comparative effectiveness research.” Yep, that’s my understanding, too.
“When used for studying a treatment with a strong placebo effect, they may make an ineffective treatment look better than an effective one.” Hmmmm, now that’s really interesting. So what you’re saying is that a treatment like acupuncture along with its ‘package of care’ may have an effect due to placebo that’s larger than the ‘package of care’ that includes the active component of a drug and it’s placebo effect combined?
You describe this phenomenon as “cinderella medicine” and I guess beauty really is in the eye of the beholder. I totally 100% agree that where you have two different ‘packages of care’ that have more than one difference between them, then a pragmatic study where one group has better results than another does not show that a particular part of one package is effective. I mean, even though the acupuncture group does significantly better time and again, this experimental design does not show that it’s down to the acupuncture. It certainly could be something else.
But it does show that one package is more effective. In other words, if you have migraines or low back pain or osteoarthritis of the knee and you want your best shot at getting rid of these ailments, you clearly know which treatment package you want to go for.
From a purely science-based medical perspective, even if the results of these studies don’t lead you to ask more pressing questions about the intervention that the group with the better outcomes received (and why wouldn’t it? Don’t you like people and want to learn more about what’s effective in making them better?), doesn’t it at least make you ask a couple of questions about the so called “science-based medical treatment” and why it’s not more effective than “SCAM” (as you so cleverly call it) in the real world? I mean, if being nice to someone for an hour a week while duping them into buying expensive woo is more effective than science-based medical drugs, with all the risks that they entail, then shouldn’t that be further explored? I mean, if you wanna be all ‘science-based’ about it?
I realise that despite the title of your “society” and the name of your blog, you hate to actually discuss science-based medicine – ironically, you’re only interested in talking about what you consider to be anything that is non-science based medicine. And I agree, that’s totally your prerogative – your blog, you decide what to write about. I have the same policy. I get it.
But, if you actually want to discredit acupuncture as total quacktastic garbage, don’t you need . . . what do they call it in science . . . a realistic comparator? If we take a condition like migraines, for example, we see in double blind RCTs that needling acupuncture points is roughly equal in effectiveness as needling non-acupuncture points and that both of these are very very effective, indeed.
Actually, for several conditions, we see that they’re actually more effective than pharmaceutical prophylactics (with a known pharmacological mechanism) which are more effective than sugar pills. And what you’re saying is that the science-based recommendation is to go to your doctor for the pharmaceuticals, even though you’re less likely to have a good outcome and simultaneously more likely to have nasty side-effects. I mean, chances are your headaches won’t go away and even if they do you’ll still feel like garbage, but no one, my friend, can call you a sucker! You showed them!
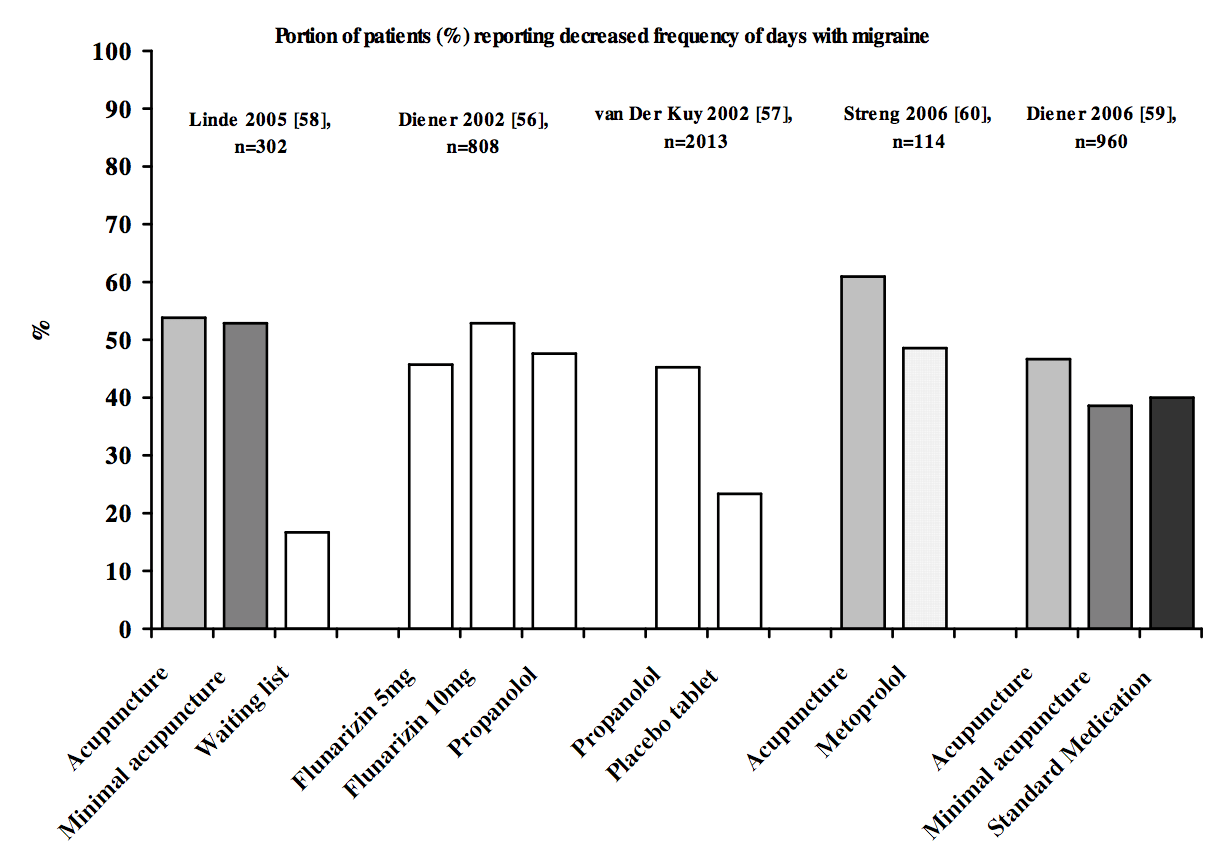
Acupuncture vs Minimal Acupuncture vs ‘Science Based Medicine’ for Migraines (Lund 2009)
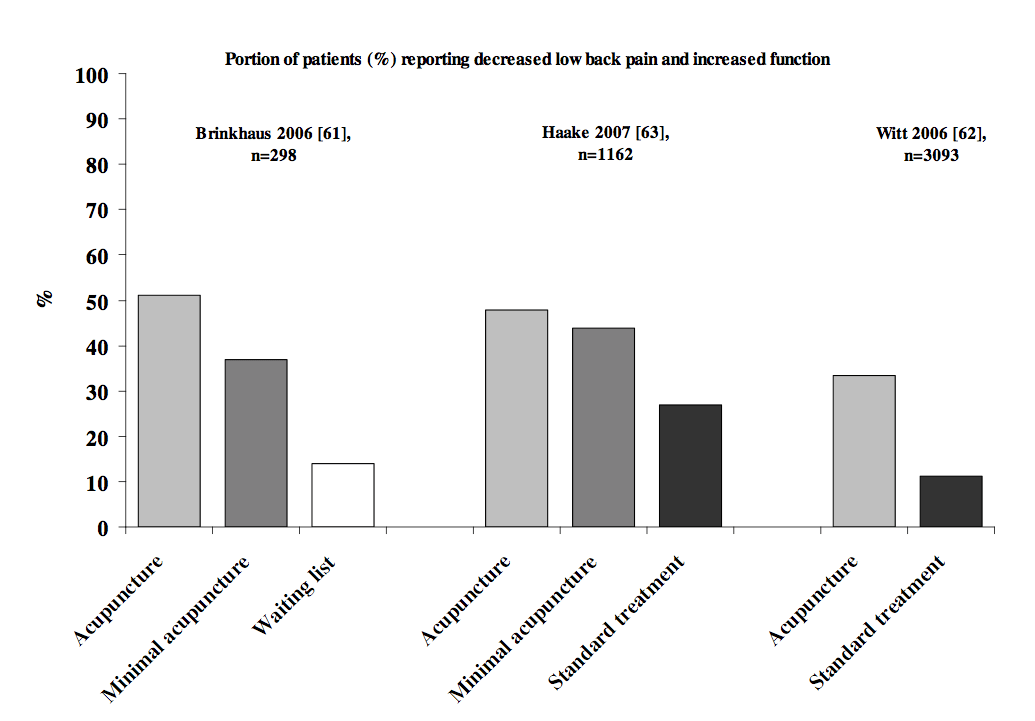
Acupuncture vs Minimal Acupuncture vs ‘Science Based Medicine’ for Low Back Pain (Lund 2009)
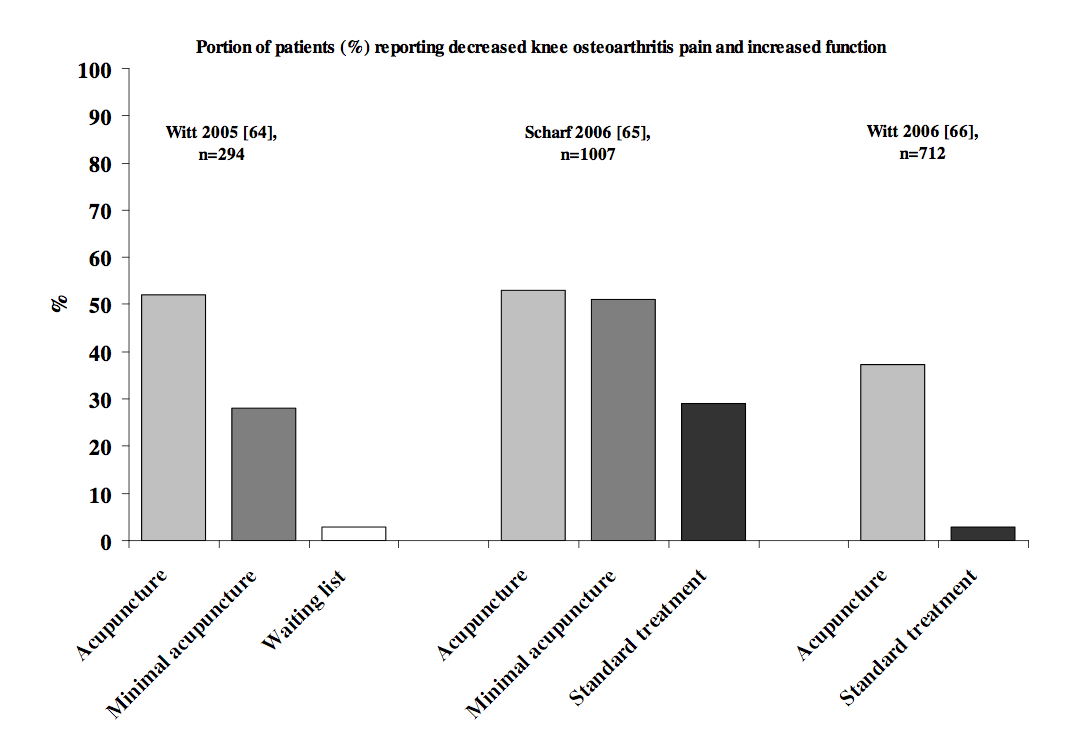
Acupuncture vs Placebo for OA of the Knee
And if you’re saying that these studies show that acupuncture doesn’t work because acupuncture and minimal acupuncture are similarly effective, what do they say about the pharmaceuticals? And how are you so confident that sticking needles in someone has no biological plausibility in preventing migraines (or that sham acupuncture is a valid placebo control12 13 14) when you haven’t even looked at the biological mechanism research?
Parting Thoughts
So these were some of the questions that I had after reading your thoughts on acupuncture. It seems like most of your qualms come from the explanatory model of qi and yin and yang. These are very interesting topics and ones that I enjoy exploring, but they are indeed separate from the more general over-arching subject of the effectiveness of acupuncture, which is a heterogenous group of techniques but mostly all involve therapeutically inserting small needles into tissue to bring about clinically beneficial effects. As you haven’t addressed the effectiveness of acupuncture as you actually define it, I’m wondering what you’re thoughts are?
Anyways, thanks again for the illuminating commentary, which is always enriching to be sure. Must get back to the needle sticking. After reading your posts, I’m considering moving away from moving qi using acupuncture and instead using the insertion of fine “acupuncture-esque” needles to affect purinergic signalling and the like, which you agree does have some scientific validity.
All the best,
Mel
1 Stener-Victorin, E., & Wu, X. (2010). Autonomic Neuroscience: Basic and Clinical. Autonomic Neuroscience: Basic and Clinical, 157(1-2), 46–51. doi:10.1016/j.autneu.2010.03.006
2 Hui, K. K., Liu, J., Makris, N., Gollub, R. L., Chen, A. J., Moore, C. I., et al. (2000). Acupuncture modulates the limbic system and subcortical gray structures of the human brain: evidence from fMRI studies in normal subjects. Human Brain Mapping, 9(1), 13–25.
3 Usichenko, T. I., Wesolowski, T., & Lotze, M. (2014). Verum and sham acupuncture exert distinct cerebral activation in pain processing areas: a crossover fMRI investigation in healthy volunteers. Brain Imaging and Behavior. doi:10.1007/s11682-014-9301-4
4 Huang, W., Pach, D., Napadow, V., Park, K., Long, X., Neumann, J., et al. (2012). Characterizing acupuncture stimuli using brain imaging with FMRI–a systematic review and meta-analysis of the literature. PLoS ONE, 7(4), e32960. doi:10.1371/journal.pone.0032960
5 Harris, R. E., Zubieta, J.-K., Scott, D. J., Napadow, V., Gracely, R. H., & Clauw, D. J. (2009). Traditional Chinese acupuncture and placebo (sham) acupuncture are differentiated by their effects on μ-opioid receptors (MORs). NeuroImage, 47(3), 1077–1085. doi:10.1016/j.neuroimage.2009.05.083
6 Wang, J.-Y., Li, H., Zhang, L., Ma, C.-M., Wang, J.-L., Lai, X.-S., & Zhou, S.-F. (2014). Adenosine as a probing tool for the mechanistic study of acupuncture treatment. Clinical and Experimental Pharmacology and Physiology, 41(11), 933–939. doi:10.1111/1440-1681.12304
7 Takano, T., Chen, X., Luo, F., Fujita, T., Ren, Z., Goldman, N., et al. (2012). Traditional Acupuncture Triggers a Local Increase in Adenosine in Human Subjects. The Journal of Pain, 13(12), 1215–1223. doi:10.1016/j.jpain.2012.09.012
8 Chung, J. W. Y., Yan, V. C. M., & Zhang, H. (2014). Effect of Acupuncture on Heart Rate Variability: A Systematic Review. Evidence-Based Complementary and Alternative Medicine, 2014(5), 1–19. doi:10.1111/j.1365-2982.2008.01164.x
9 Anderson, B., Nielsen, A., McKee, D., Jeffres, A., & Kligler, B. (2012). Acupuncture and Heart Rate Variability: A Systems Level Approach to Understanding Mechanism. Jsch, 8(2), 99–106. doi:10.1016/j.explore.2011.12.002
10 Jia, J., Yu, Y., Deng, J.-H., Robinson, N., Bovey, M., Cui, Y.-H., et al. (2012). A review of Omics research in acupuncture: The relevance and future prospects for understanding the nature of meridians and acupoints. Journal of Ethnopharmacology, 140(3), 594–603. doi:10.1016/j.jep.2012.01.034
11 Langevin, H. M. (2014). Acupuncture, connective tissue, and peripheral sensory modulation. Critical Reviews in Eukaryotic Gene Expression, 24(3), 249–253.
12 Lundeberg, T., Lund, I., Sing, A., & Näslund, J. (2011). Is Placebo Acupuncture What It Is Intended to Be? Evidence-Based Complementary and Alternative Medicine, 2011(1), 1–5. doi:10.1016/S0140-6736(97)10471-8
13 Lund, I., Näslund, J., & Lundeberg, T. (2009). Minimal acupuncture is not a valid placebo control in randomised controlled trials of acupuncture: a physiologist’s perspective. Chinese Medicine, 4(1), 1. doi:10.1186/1749-8546-4-1
14 Lundeberg, T., & Lund, I. (2007). Are reviews based on sham acupuncture procedures in fibromyalgia syndrome (FMS) valid? Acupuncture in Medicine, 25(3), 100–106.